Happy Memorial Day from Littleton!
This was another busy week, but full of a lot of interesting cases. We started out our week with our Monday Morning Meeting going over ophthalmology from Dr. Lori, and got a good refresher on some of the most common problems we might run into as equine veterinarians. We also had an interesting Journal Club session with the interns on Tuesday, going over a paper on the differences of using triamcinolone, a steroid, for joint injections vs triamcinolone and hyaluronic acid (HA), which is a really common combination to use. The study found that the combination didn't provide any significant improvements or added benefits than just the steroid alone. There were some simple flaws with the set up of the study, in that this couldn't really be a blind test, as the two cannot be combined in a single injection. Another problem we discussed was the lack of vet assessment 3 months post-treatment, it was just a simple questionnaire/phone call discussion about the owners' perceptions of their horse. This can lead to some obvious subjectivity, so we thought that it could lend better in future studies to have consistent evaluation throughout. Yet, it was thought provoking, seeing as a lot of owners ask about the injections and the added benefits of combining the two or not, as well as the added cost, so it was interesting to get to work through some of the pros and cons. I think the overall consensus was to still offer the two, and just explain to the owners the effects or results that have been potentially found.
As far as other cases from the week, the surgery suite was fairly busy. We had a 1 1/2 month old foal in for a transphyseal bridging for the treatment of his severe angular limb deformity (ALD). There was about an 18 degree carpal valgus deviation so the bridges were placed laterally to stunt the growth on the outside, and all the medial aspects to catch up a bit. They will go in and remove those once the legs appear straightened out, or else it can lead to an over-correction. There were also a couple arthroscopies as well.
A horse that has been with us for about a week and a half who presented as a choke, has had a few more scopes to try to figure out what to do and what's going on in this poor guy's larynx. He initially had a tracheostomy performed, and has been on tubed electrolytes/fluids, as every time he went to eat he was still having food coming back out his nose. He finally has been able to move to some mashes and wet down hay, slowly working back to normal food. On one of the early scopes, it was debated if he had an entrapped epiglottis, and action needed to be taken. He eventually had a laser vocal cordectomy done, and while it wasn't wholly successful, it has shown improvements, albeit slowly. The epiglottis is going through a bit of a necrotic and swollen phase, but will eventually slough off and lead to restoration of his airway, hopefully. He's hanging in there though!
Another fun case was a 10yo QH barrel racer who came in with some lameness issues. The previous rads from the referring DVM showed some fusion in his hocks, mostly on the left side, in the DIP joint. It was decided that both would be injected though. Once some flexion tests were done, there was revealed some soreness on the front end as well, around the navicular areas on both fronts. Dr. French decided to get some radiographs of his front feet, just to make sure, and on his right front, there showed a definite fracture of the navicular bone! It did look older/more chronic just based on the fact that there was remodeling already happening. Yet, just to cover all the bases, the coffin joint got injected as well. The horse received os-phos too, on top of it all, in order to help with some/any bone bruising or edema present. It will be interesting to hear how he does with this further treatment.
Finally, I went out into the field on Friday with Dr. Senn for a facial laceration repair. Thankfully, this big old 6yo TB sweetheart must've just done it, as it was fresh and still bleeding. We knew that was a good sign at least. After a load of antibiotics, cleaning it up and lavaging it out, there were no distinguished pockets anywhere, again, a great sign. So, keeping our sterile field, Dr. Senn sutured him all up, a couple vertical mattresses for tension/support and some simple interrupteds to close it all up. She debated to leave a little triangle for drainage, but in the end closed it up, allowing some space for drainage, but wanting to avoid any further potential infection. All was well!
Also, this weekend I had the chance to host one of my classmates, Lauren Lauwers, out in Denver! It was a lot of fun, and was really nice to have the ability to get out a bit and experience some of what Colorado has to offer. I hope everyone had a great weekend and look forward to another exciting week!
Taylor
Monday, May 30, 2016
Week 1 and 2 from Brown Equine Clinic
It's been a whirlwind - probably not much different than what you are all experiencing. Brown Equine Clinic is very busy with standard bred racing horses. We do lots of lameness exams, radiographs, and injections. I've seen a handful of ventriculocordectomies at Brown Equine hospital. The goal of this procedure is to improve the breathing of a horse with left recurrent laryngeal nerve paralysis. A tie back can improve the breathing of the horse but costs more and puts the horse at risk because they must be under anesthesia. To do the procedure, we have the horse in stocks, sedated with the head supported. The larynx is doused with carbocaine, which lasts longer than lidocaine in the event that the surgery takes longer than predicted. We do a line block on the skin beneath the larynx with lidocaine and make an incision through the tissues to the cricothyroid membrane. With help from an endoscope passed nasally, we can remove the ventricular saccules and vocal cords. When this scar tissue forms it makes the arytenoids stiffer so that the horse can breathe more efficiently. This is important for draft horses who do not handle anesthesia very well. I've seen more of these surgeries performed on the big guys in general. Per Dr. Brown, he sees an improvement rate of about 90%. No pictures because I get to guide the endoscope and my hands are pretty busy!
-Brandi
Week 2 in the Ambulatory department of Rood & Riddle
These last two weeks have gone by so quickly. Just about every day has been more than 8 hours, but it doesn't seem like it. We're always moving, always doing something. Even on the "slow" days, we still have several hours of work and we go at the usual speed to have a little more time off. At this point, I'm loving every minute of it!
Sunday was a sad day. We lost two foals overnight. I rode with Dr. Friend and the other student. Our day went pretty smoothly despite the rough night for a couple clients. We started treating another foal that was starting down the same path. I learned that threading a needle for a Caslicks procedure is not quite as straightforward as it sounds. The suture has to be fed through the loop twice so that it is secured to the needle and will not fall off as the doctor manipulates the suture. We went out for breakfast at noon and palpated our last mares 1 p.m.
Monday was another early start with Dr. Jordan Kiviniemi-Moore. The morning started out with us washing out a 45 day old aborted fetus. We were able to see the little sacs that protect it as it grows. Unfortunately, it had been dead for a few days and had deteriorated a lot, so we weren't able to see what the little critter had looked like. I was able to place a couple lavage tubes myself later in the day and run the fluid. These are done to wash out the uterus either before breeding to make sure it is a clean environment for the semen or after breeding to get out the semen that didn't make it up to the oviduct to fertilize the egg. As it turns out, semen is irritating to the uterus and can prevent a pregnancy from being retained. This is an even larger risk when doing artificial insemination because there is usually extender added to the semen. The extender used for frozen semen is the most irritating. The post-breeding treatments can be done as early as four hours after breeding and can continue for up to five days. At the five day mark, the embryo will arrive into the uterus. At this time, it is no longer safe to do lavages without being set up to catch an embryo for transfer to a recipient mare. Back to the day's events. Towards the end of the day, I watched Jordan remove a pair of wolf teeth. The roots were much longer than expected. Unfortunately, there wasn't much space so I couldn't really tell what she was doing in there. We also ran a couple bags of fluids to a mare that had tied up during her training session earlier that day. We only did a small percentage of the fluids that would have been run to her in the hospital setting. Unfortunately, we were in the barn setting and did not have the time of equipment to run the proper treatment. We decided that it was better to do part of the fluid treatment than none. Our last stop was an emergency diarrhea foal. He and his momma were both a handful! We placed a catheter, ran a liter of fluids, and administered a cocktail of medications. The owners did not feel comfortable doing this on their own, so we saw them twice a day for the next few days. Monday was my first late night. I got home at 11 p.m. and started Tuesday at 5 a.m.
Tuesday was another long day. I got home at 10 p.m. after the 5 a.m. start. We found several little black dots (early pregnancies) which allowed for a good start to the day. I did several blood draws and got to operate the ultrasound probe for a lung scan. During a vaccination appointment, we diagnosed a case of bilateral fibrotic myopathy- part of the muscle in the back of the hind legs had become fibrotic and lost their elasticity. This leads to the horse having a tell-tale gait abnormality. Unfortunately, we had to advise the client not to sell the horse for a long trail horse because the lack of elasticity makes walking take more effort than it should. We were sent out on a colic emergency. It turned out to be an older mare with cellulitis in one of her hind limbs. This had led to a fever and dehydration. These are suspected to have caused the drier stool and mild impaction colic. We gave some drugs, palpated, refluxed, gave oral fluids, and sweat wrapped both hind legs to pull the edema out.
I had Wednesday off, so I slept in. It was really nice outside, so I sat on the porch and played on the internet for a while. I have collected a list of local restaurants to try out, so I found one for dinner. Vinaigrette Salad Kitchen was a tasty choice. They have soups, salads, and signature lemonades. Unfortunately, the lemonades had already been cleaned up for the day. The soup and salad I had were delicious though. I had to stop by Walgreen's and get some allergy medicine. My nose was starting to run like crazy! Overall, a very relaxing day.
Thursday, I was back to the grind with Jordan. We started a tad later and ended a little earlier than we had at the beginning of the week. The day was pretty routine until we were called out to look at a lame horse. Jordan found a heel bulb abscess and wrapped the foot up to help soften the tissue to allow it to pop and relieve the pressure. The sad part of the day was that we missed the castration party because the time kept getting moved on us. It's starting to be difficult for me to remember what days things are happening because we are doing so much. Some days we feel like we've just been driving in circles and don't realize how much we've done until we get to the clinic to restock the truck and do the billing paperwork. Even thiough it gets boring to wash lavage tubs, make up the cotton, and mix more DMSO flushes, that's when I really see how much we've done. Then Jordan shows me the stack of bills that she has finished annotating. It makes me happy that we are doing so much without realizing it.
Friday, Jordan had an ambulatory intern party in the evening, so we tried to keep it to an early finish. We moved along at a good pace and had even finished a bit early. Of course, that's when you get silly emergency calls. This client had called for lacerations, but the horse just had a few skinned spots on its legs. Nothing major at all. Jordan wrapped the legs just to make them happy that we had done something other than just give Bute.
Saturday- end of week 2... Saturday felt almost like two days instead of one. I rode with Jordan. We moved at a pretty quick pace to get as much done as we could before she had to go work the show at the Horse Park. The morning was very routine. She dropped me off just in time to get to the Horse Park at 11 a.m. I only worked about four hours. That left plenty of time off. When I woke up from my nap, I was startled by the AC repairman outside the hallway window. After he fixed our cooling problem, I went to the store for some more groceries. It took much longer than I expected to work out doing laundry at the neighbor's. I'm glad most of my chores got done. Laundry still needs to be put away, but at least it's clean.
That marks the end of my second week! Even though the hours are rough and causing me to run back into the caffeinated world, I wouldn't trade it. I still have a long way to go, but I think this will be a very enjoyable summer.
Week 3 @ Cleveland Equine Clinic
This week has been a busy one and full of surgeries and colics.
I have been helping care for the colicing horses that are currently in the clinic, both with impaction colics. Treatments for each of the horses have been quite similar. Treatments include, hydrating them by using an NG tube to deliver fluids to their stomachs, and feeding mashes and small amounts of hay. One horse also has received IV fluids based on the severity of his impaction and the necessity to provide him with more fluids than NG tubing could. Often electrolytes or epsom salts are added to the fluids that are being pumped into their stomachs. This helps not only with hydration but also aids to draw in water from interstitial fluid into the gut. The goal is to provide enough fluids to hopefully soften the impaction to help the horse in passing it through. Positive signs of the impaction resolving are passing manure, drinking water, and regaining GI sounds as well as comfort.
One amazing surgery I had the chance to observe was a repair of a rectovaginal tear. The tear occurred due to the mare aborting and having a traumatic foaling. For these repairs you must wait until the tissue swelling and inflammation goes down. Due to the location of the repair, you also must ensure that the horse has relatively soft stool before and after the surgery. This is important so that after the reconstruction is complete there will be minimal straining to defecate. For this the mare was kept on pasture from the time of the tear until surgery, as to soften her manure. The surgery is by no means sterile or even aseptic, but prepping consists of trying to clear away as much manure and dirt as possible from the site. First incisions are made along the angle of where the rectum once was. This is done to create a "raw" edge that can be sutured to the opposing side's edge. For those of you who are familiar, this is the same idea behind the tissue scoring done for a caslicks procedure. In this case when these edges heal together, there will be a rectum and vestibule. 2 Vicryl was used in a modified mattress suture pattern. The vulva was repaired with 1 prolene in a simple interrupted pattern.
 Before--as you can tell there is no separation between rectum and vestibule.
Before--as you can tell there is no separation between rectum and vestibule.
 This is blurry- but this is how she looked before any incisions were made. There is a slight shelf of tissue that exists, the goal is to extend that shelf and separation to create two openings. The rectal mucosa is also used as a landmark of where the rectum vs. vestibule is located.
This is blurry- but this is how she looked before any incisions were made. There is a slight shelf of tissue that exists, the goal is to extend that shelf and separation to create two openings. The rectal mucosa is also used as a landmark of where the rectum vs. vestibule is located.
 In this image the surgeon is creating a fresh edge of tissue to form the perineal body.
In this image the surgeon is creating a fresh edge of tissue to form the perineal body.
 The surgeon is suturing the fresh edges of rectal mucosa together to form the rectum.
The surgeon is suturing the fresh edges of rectal mucosa together to form the rectum.
 Nearing the end of the procedure, tissues start to be in a normal anatomical placement. A rectum and anal sphincter can be seen, however it should be noted that the anal sphincter cannot be repaired (but the horse lives outside or in a stall--so there is no true need for continence.)
Nearing the end of the procedure, tissues start to be in a normal anatomical placement. A rectum and anal sphincter can be seen, however it should be noted that the anal sphincter cannot be repaired (but the horse lives outside or in a stall--so there is no true need for continence.)
 After surgery- she may not be as symmetrical as she once was, but there is now a true separation between rectum and vestibule. Thoroughbred breeding requires live cover and does not allow for AI, therefore a caslicks was not done at this time--however could have been done if there were no breeding restrictions. Once in foal again, she will most likely receive a caslicks to prevent any contamination of fecal material into her vagina.
After surgery- she may not be as symmetrical as she once was, but there is now a true separation between rectum and vestibule. Thoroughbred breeding requires live cover and does not allow for AI, therefore a caslicks was not done at this time--however could have been done if there were no breeding restrictions. Once in foal again, she will most likely receive a caslicks to prevent any contamination of fecal material into her vagina.
I am so happy to be at Cleveland Equine this summer, and I am learning so much from all of the doctors and staff. I am thankful for this opportunity to take part in such a wonderful practice and experience!!!
-Roya Oliai
I have been helping care for the colicing horses that are currently in the clinic, both with impaction colics. Treatments for each of the horses have been quite similar. Treatments include, hydrating them by using an NG tube to deliver fluids to their stomachs, and feeding mashes and small amounts of hay. One horse also has received IV fluids based on the severity of his impaction and the necessity to provide him with more fluids than NG tubing could. Often electrolytes or epsom salts are added to the fluids that are being pumped into their stomachs. This helps not only with hydration but also aids to draw in water from interstitial fluid into the gut. The goal is to provide enough fluids to hopefully soften the impaction to help the horse in passing it through. Positive signs of the impaction resolving are passing manure, drinking water, and regaining GI sounds as well as comfort.
One amazing surgery I had the chance to observe was a repair of a rectovaginal tear. The tear occurred due to the mare aborting and having a traumatic foaling. For these repairs you must wait until the tissue swelling and inflammation goes down. Due to the location of the repair, you also must ensure that the horse has relatively soft stool before and after the surgery. This is important so that after the reconstruction is complete there will be minimal straining to defecate. For this the mare was kept on pasture from the time of the tear until surgery, as to soften her manure. The surgery is by no means sterile or even aseptic, but prepping consists of trying to clear away as much manure and dirt as possible from the site. First incisions are made along the angle of where the rectum once was. This is done to create a "raw" edge that can be sutured to the opposing side's edge. For those of you who are familiar, this is the same idea behind the tissue scoring done for a caslicks procedure. In this case when these edges heal together, there will be a rectum and vestibule. 2 Vicryl was used in a modified mattress suture pattern. The vulva was repaired with 1 prolene in a simple interrupted pattern.






I am so happy to be at Cleveland Equine this summer, and I am learning so much from all of the doctors and staff. I am thankful for this opportunity to take part in such a wonderful practice and experience!!!
-Roya Oliai
Sunday, May 29, 2016
Hello from Equine Analysis Systems!
Hey everybody!
I have just finished up my first few weeks at Equine Analysis Systems (EAS) and can't wait to tell you all what I've been up to. My summer experience will be slightly different than my fellow students' as EAS is more of a research based company and doesn't practice clinical equine medicine. EAS focuses on optimizing the individual racing performance of racing thoroughbreds and does so with a variety of technologies they have developed. These technologies include a heart scan, conformational analysis, a wind test, motion test, and metabolic analysis. If you would like to learn more about these specific technologies please visit their website at www.equineanalysis.com.
EAS has a team of 4 veterinarians, 4 techs, and a few other staff members. It is a very close knit company and everybody has made me feel very welcomed and has helped to integrate me into the company. They have even created a special project just for me focusing on upper airway pathology. I will be comparing the pathology of sound with visual pathology at rest. To do this, I will be working most with the wind test, which records the horse's breathing while they run, and analyzing that data for any upper airway pathology. This test can pick up and record noises produced by pathology before we can audibly detect them. Then after the horse works, we will use video endoscopy to see if we can visually detect any pathology of the upper airways. We have had a few issues with getting our scope working so stay tuned to see what we find this summer!
On a typical day of track testing, we drive to Churchill Downs, and get started on getting all of our equipment on the horses that will be working that day. It has been an amazing experience to get to work on the backside of Churchill Downs and such a privilege to be able to collect data on these supreme equine athletes. I have never seen horses so fit and clean in my entire life! After the data is collected we head back to the office and analyze the data. I usually help run the blood work and am still learning how to analyze the sound files from the wind test. One of the coolest parts is getting to watch the GoPro videos that the jockeys wear. The jockeys wear the video as they work the horse and watching them is like riding around the Churchill track yourself!
On days that we aren't track testing, I am either analyzing data, prepping for the next track test, or learning about the other technologies they use. I am learning so much about equine physiology and how all of their systems work together to produce this extreme athlete. I have also gotten to practice some clinical skills on the veterinarians' own horses. Whenever they have vet work that needs to be done on their horses, I am always welcome to come help out. So far I have been able to practice drawing blood, giving vaccines, and trans-cervically infusing a mare with antibiotics.
Also, Lexington is just beautiful in the summer time! My drive to work is through the backroads surrounded by green pastures and lined with trees. It is such welcome site after being stuck in classroom all year. It is definitely a wonderful place to spend your summer! It has also been great to be exposed to another field of equine medicine that I wasn't aware of before. You still get plenty of hands-on time with horses but have more regular hours. It could be a great career choice for those that love equine medicine but don't relish the emergency/ on-call lifestyle. Hopefully, I'll have some pictures to share by my next post. Once our scope starts working, I might even have a few cool shots of the larynx!
I have just finished up my first few weeks at Equine Analysis Systems (EAS) and can't wait to tell you all what I've been up to. My summer experience will be slightly different than my fellow students' as EAS is more of a research based company and doesn't practice clinical equine medicine. EAS focuses on optimizing the individual racing performance of racing thoroughbreds and does so with a variety of technologies they have developed. These technologies include a heart scan, conformational analysis, a wind test, motion test, and metabolic analysis. If you would like to learn more about these specific technologies please visit their website at www.equineanalysis.com.
EAS has a team of 4 veterinarians, 4 techs, and a few other staff members. It is a very close knit company and everybody has made me feel very welcomed and has helped to integrate me into the company. They have even created a special project just for me focusing on upper airway pathology. I will be comparing the pathology of sound with visual pathology at rest. To do this, I will be working most with the wind test, which records the horse's breathing while they run, and analyzing that data for any upper airway pathology. This test can pick up and record noises produced by pathology before we can audibly detect them. Then after the horse works, we will use video endoscopy to see if we can visually detect any pathology of the upper airways. We have had a few issues with getting our scope working so stay tuned to see what we find this summer!
On a typical day of track testing, we drive to Churchill Downs, and get started on getting all of our equipment on the horses that will be working that day. It has been an amazing experience to get to work on the backside of Churchill Downs and such a privilege to be able to collect data on these supreme equine athletes. I have never seen horses so fit and clean in my entire life! After the data is collected we head back to the office and analyze the data. I usually help run the blood work and am still learning how to analyze the sound files from the wind test. One of the coolest parts is getting to watch the GoPro videos that the jockeys wear. The jockeys wear the video as they work the horse and watching them is like riding around the Churchill track yourself!
On days that we aren't track testing, I am either analyzing data, prepping for the next track test, or learning about the other technologies they use. I am learning so much about equine physiology and how all of their systems work together to produce this extreme athlete. I have also gotten to practice some clinical skills on the veterinarians' own horses. Whenever they have vet work that needs to be done on their horses, I am always welcome to come help out. So far I have been able to practice drawing blood, giving vaccines, and trans-cervically infusing a mare with antibiotics.
Also, Lexington is just beautiful in the summer time! My drive to work is through the backroads surrounded by green pastures and lined with trees. It is such welcome site after being stuck in classroom all year. It is definitely a wonderful place to spend your summer! It has also been great to be exposed to another field of equine medicine that I wasn't aware of before. You still get plenty of hands-on time with horses but have more regular hours. It could be a great career choice for those that love equine medicine but don't relish the emergency/ on-call lifestyle. Hopefully, I'll have some pictures to share by my next post. Once our scope starts working, I might even have a few cool shots of the larynx!
Wednesday, May 25, 2016
Hello from Littleton Equine!
Hey guys! Just updating from my first week, Sorry for the delay, had to wait to see if I had approval for sharing some pictures!
This past week has been awesome, and I'm sure just like everyone else, it's been a lot of trying to get adjusted to the system and how everything operates. Littleton Equine has 16 total doctors, and 4 interns, along with techs and assistants for each. My primary roles thus far have consisted of a lot of ICU training. These will be my first couple weeks, then I will branch out and go with different doctors throughout the practice. There is also a Summer Show Series starting up at the large Colorado Horse Park that I will be attending, accompanying either a doctor or intern out there..! Also, every Monday morning, we have a topic presented by one of the doctors, last week was Cardiology (fitting for my fellow 3rd years haha) and that's followed by the rundown of good cases from the previous week. It's really fascinating to hear all of the knowledge that they all exhibit. Tuesday mornings, we are able to sit in on the interns' Journal Club, where one of them pulls an article from a journal and there's a general overview and discussion about it.
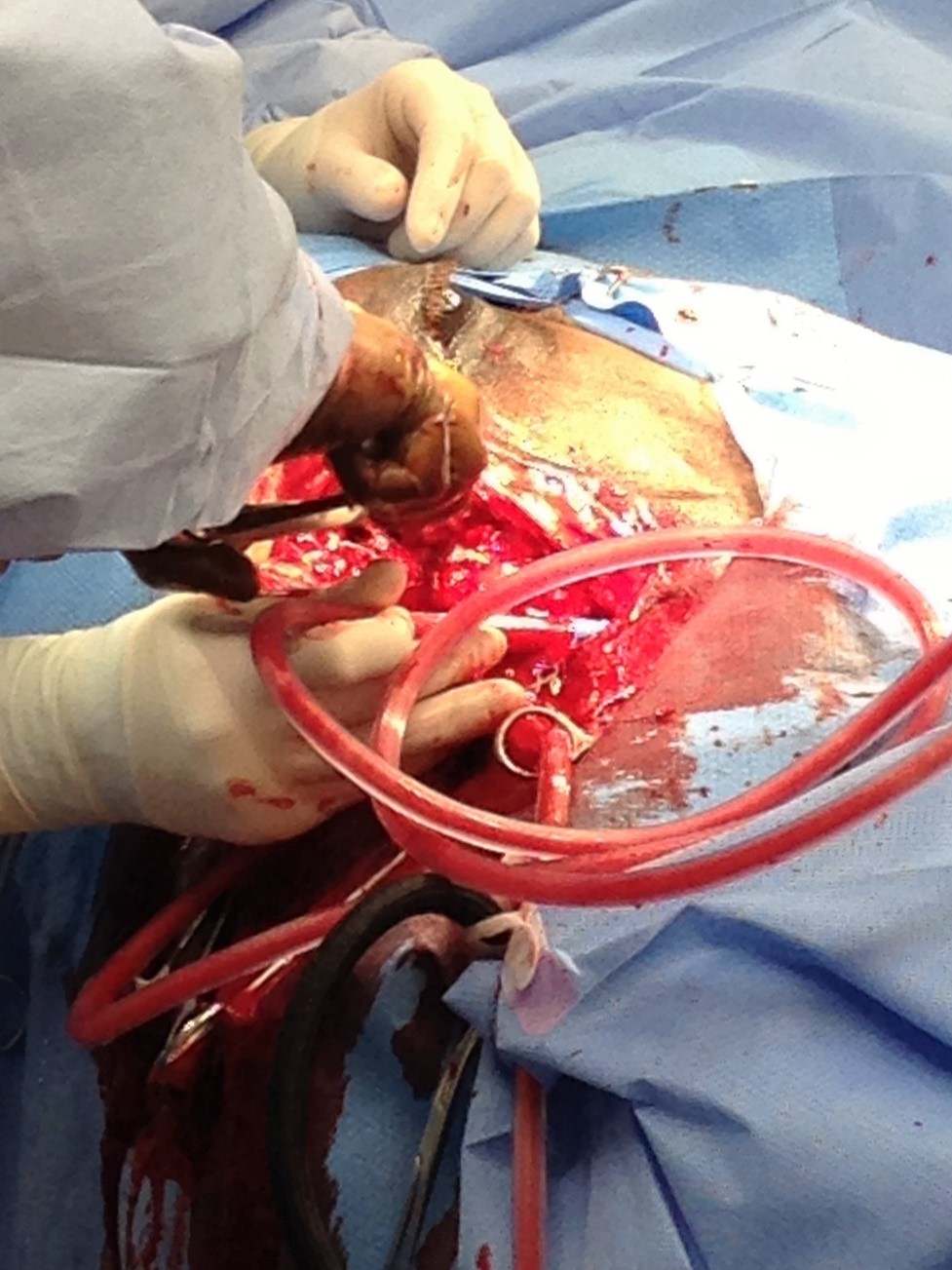
I have been able to be a part of some really cool operations and work ups in the hospital as well. There have been about a million and one colics since I've arrived, as I'm sure many of you are experiencing as well. Colorado is a very dry climate and predominantly a desert atmosphere, so sand colic is really big out here unfortunately. I have also been able to help with a handful of lameness exams, ultrasounds, radiographs, etc. There are so many doctors and so many things going on at one given time, that the opportunity to see some really interesting cases is always present. We had one horse present as a colic, but was progressively getting worse. Basically every test was thrown at him, he had all the bloodwork, a belly tap, ultrasounds, rads, the whole nine. He had a persistently increasing white cell count, so they were obviously worried about inflammation or an infection of some sort. Unfortunately, nothing conclusive was found and the decision was made to euthanize him. I was able to be there for that, and they found some pretty incredible results.
This entire liver lobe was completely obliterated, one massive abscess had just destroyed it. As you can see, the doctor is able to put his hands completely through the entire lobe..
This is just another view laid out, showing the extent of the abscess.
There was a small adhesion on the ventral colon, but it was unsure if that resulted from the liver abscess or if that was the initial cause which led to a hematogenous spread to the liver. Although, the necropsy was deemed a good decision, seeing as trying to remove that much liver would have been impossible.
We also had a couple surgeries in this week, one in particular was an emergency lameness, so took the horse into a pastern joint arthroscopy. Since it was an emergency, I was able to take on more a role of anesthesia assistant, which was really great getting some hands on experience with that. On ultrasound, there seemed to be some adhesion within the superficial digital flexor sheath that they were concerned about. The horse had just previously had this same joint scoped about 5 weeks prior up at Colorado State, but was brought here for time circumstances. Once they were in and found the potential areas of adhesion, it was all taken care of and removed, and all was successful.

I apologize for the sideways pictures, I will try to figure out how to change that for next week..! Other than that, it has been an awesome summer so far. Excited to see where the rest of these weeks go, and can't wait to hear about everyone else's as well!
-Taylor
Sunday, May 22, 2016
Week 1 with Equine Athlete!
Hey everyone, I had a first great week working in Mantua, Ohio with Dr. Hill and his associate from Texas, Dr. Bush. I had a short week, working one overnight trip. We spent both days at a world class, full service barn that houses over 200 Arabian and Saddlebred show horses. This trip was a great introduction to the horses I will be working with and around this summer. It's so interesting being exposed to yet another equine discipline and style! The first day out I learned how to set up the portable ultrasound, radiograph, and shockwave machines. I also learned how to prep and scrub for joint injections. On the second day I got to watch some horses "go" with Dr. Hill as he performed lameness exams, and then I got to watch the follow-up treatments performed by Dr. Bush. Most of the joint injections performed were to the fetlocks, hocks and stifles, as well as ultrasound guided sacroiliac injections. We also radiographed a horse with a navicular bone fracture and a horse with abscesses in both hind feet. It was a great experience learning how to hold the plate for all the different views. This week I'll be on the road to Columbus, Ohio heading to my first show experience with Dr. Hill at the Buckeye Sweepstakes! Hope everyone is enjoying their experiences as much as I am!
Alex
Alex
Weeks 1 & 2 at Cleveland Equine Clinic LLC
Thus far my experience has been amazing! All of the doctors and staff work together to provide top notch medicine and diagnostics.
I have been exposed to more lameness cases in the first week here than I have ever seen. Watching Dr. Genovese work is a very humbling experience. With over 40 years of equine lameness experience he is able to pin-point lamenesses with just a few jogs of the horse. I am only just starting to learn how to watch every part of the horse on each jog, and listen for lameness with the sound of each hoof strike. Seeing such a large lameness caseload has helped me start to recognize some gait abnormalities, palpate limbs, and identify radiographic changes as well. The clinic also uses a tool called Lameness Locator to help diagnose the more subtle lamenesses, those that sometimes only the rider can feel. It works by placing three inertial sensors on the horse; on the head, above the pelvis, and on the right front pastern. The horse is then jogged 4 times up and down the lameness work up area outside. The data from the sensors are sent to and processed by a tablet, from this we are able to see if there is an impact or push off lameness and in which foot. The data helps then determine the next step, radiographs or nerve blocks or other options. Blocking out part of the affected limb can help determine where in that leg the lameness is. By performing regional carbocaine nerve blocks at certain diagnostic sites, the horse is unable to feel from the bock distally. Therefore if the problem is distal to the nerve block, when jogged again the horse will improve greatly. I will definitely continue to learn and absorb all I can, my goal is to be able to identify lamenesses by the end of the summer.
I have also been with a variety of the ambulatory doctors. With the end of breeding season approaching there is still some reproduction work to be done. This includes culturing mares, flushing, inseminating, and ovulation checks. There are also some foals that we've seen to do a basic physical and IgG check to ensure there has been proper colostrum consumption and passive transfer. We have injected joints and I've helped scrub hocks, coffin joints, and more!
Just this week we had two miniature ponies come in the clinic for some work. We extracted a tooth from one, which was a difficult job, as the tooth was the size you would find in an average horse but stuck in the maxilla of a mini. The next one got his teeth floated and was castrated. This was an amazing experience for me, as I was able to actually participate in the castration! Under supervision of the Dr. I stripped away the tunica albuginea over one of the testicles for the open castration! This Saturday has also been busy. A horse came in with colic and has been staying at the clinic. I was able to help take the physical exam, and hold for NG tubing. I was also given the chance to palpate him and feel some of the colon, though I will definitely need more practice with that skill. Late last night we also ultrasounded him to see if there were any other abnormalities, and after the initial exam I was able to practice finding some of the organs.
I am learning so much for all of the doctors, technicians, and staff, and am so appreciative of all of their expertise and time to teach me! I could not have asked for a better summer experience. Everyone at the clinic is amazing and very skilled, I am honored to have the opportunity to be a part of their clinic this summer.
I have been exposed to more lameness cases in the first week here than I have ever seen. Watching Dr. Genovese work is a very humbling experience. With over 40 years of equine lameness experience he is able to pin-point lamenesses with just a few jogs of the horse. I am only just starting to learn how to watch every part of the horse on each jog, and listen for lameness with the sound of each hoof strike. Seeing such a large lameness caseload has helped me start to recognize some gait abnormalities, palpate limbs, and identify radiographic changes as well. The clinic also uses a tool called Lameness Locator to help diagnose the more subtle lamenesses, those that sometimes only the rider can feel. It works by placing three inertial sensors on the horse; on the head, above the pelvis, and on the right front pastern. The horse is then jogged 4 times up and down the lameness work up area outside. The data from the sensors are sent to and processed by a tablet, from this we are able to see if there is an impact or push off lameness and in which foot. The data helps then determine the next step, radiographs or nerve blocks or other options. Blocking out part of the affected limb can help determine where in that leg the lameness is. By performing regional carbocaine nerve blocks at certain diagnostic sites, the horse is unable to feel from the bock distally. Therefore if the problem is distal to the nerve block, when jogged again the horse will improve greatly. I will definitely continue to learn and absorb all I can, my goal is to be able to identify lamenesses by the end of the summer.
I have also been with a variety of the ambulatory doctors. With the end of breeding season approaching there is still some reproduction work to be done. This includes culturing mares, flushing, inseminating, and ovulation checks. There are also some foals that we've seen to do a basic physical and IgG check to ensure there has been proper colostrum consumption and passive transfer. We have injected joints and I've helped scrub hocks, coffin joints, and more!
Just this week we had two miniature ponies come in the clinic for some work. We extracted a tooth from one, which was a difficult job, as the tooth was the size you would find in an average horse but stuck in the maxilla of a mini. The next one got his teeth floated and was castrated. This was an amazing experience for me, as I was able to actually participate in the castration! Under supervision of the Dr. I stripped away the tunica albuginea over one of the testicles for the open castration! This Saturday has also been busy. A horse came in with colic and has been staying at the clinic. I was able to help take the physical exam, and hold for NG tubing. I was also given the chance to palpate him and feel some of the colon, though I will definitely need more practice with that skill. Late last night we also ultrasounded him to see if there were any other abnormalities, and after the initial exam I was able to practice finding some of the organs.
I am learning so much for all of the doctors, technicians, and staff, and am so appreciative of all of their expertise and time to teach me! I could not have asked for a better summer experience. Everyone at the clinic is amazing and very skilled, I am honored to have the opportunity to be a part of their clinic this summer.
Week one at Oakridge Equine!
Week One at Oakridge Equine in Oklahoma!
My first week started off well here in Oklahoma. As usual, I spent my first few days just getting to know the veterinarians and staff and how the hospital runs. This is a very busy practice that has 5 full time veterinarians, one resident and five interns. The caseload is very heavy and diverse, with everything from mandibular fractures, neurologic cases, orthopedic surgeries, colics, pneumonia, lameness evaluations, pre-purchase exams and everything inbetween.
My day starts around 6:30am with morning treatments for the hospital patients. Our first appointments start at 8am and run until 6pm. As I learn the system and where things are, I mostly observe and jump in whenever I see a chance to help out.
The clinic has two barns with about 60 stalls. There is two surgery suites, one for soft tissue and one for orthopedics, a radiology room, an MRI machine, two exam rooms, two indoor lameness areas, four ICU stalls and three isolation stalls. I am currently living above the clinic in the extern apartment, but I will move next week, most likely to an extra apartment of one of the veterinarians, when more externs start arriving.
This weekend I also had the opportunity to sit in on a joint injection lab for the equine practitioners in the surrounding area. It was a great learning experience and anatomy refresher!
I haven’t nailed down the details about posting pictures yet, but once I get the okay to post I will add some to my future posts!
Thanks for reading!
Sarah
Weeks 1 and 2 RREH Surgery
When you first show up to work as a surgery tech at Rood and
Riddle, you may think you have a good idea of what goes on each day in the
hospital. Your preconceived notions may even be somewhat true, but you can’t
truly understand how it all happens until you’ve gotten your hands dirty and
participated in the organized intensity that sees as many as 20 or more horses
undergo surgery in a single day. I immediately realized this the first day on
the job. When you arrive you know what your job is; you know that you’re
supposed to help out…but your primary focus becomes trying to wrap your mind
around the orchestration of it all while you do your best to stay out of the
way. This was essentially my first day-the smell of the horses mixed with a
multitude of cleaning products, the sounds of the hoist raising and dropping
horses, and the acute awareness of what is sterile (do not touch!!!) and what
isn’t. As the hours and days moved on, I gradually became more involved and
started to develop an idea of how the day is actually organized. The horses
scheduled for surgery are written up on the board (some are scheduled and some
are added as emergencies). The surgeon operating on the horses adds a number to
the board next to each horse as the order in which they will be operated on
becomes clear. The horse with the next number is retrieved, dropped in a
recovery stall and hoisted onto a surgery table. The surgical site is clipped
(most of the time) and prepped, generally with a rough and a sterile scrub.
Once the sterile scrub is complete, the horse can be moved into the surgery
suite and the surgery can begin. At this point other surgery techs have begun
to retrieve and prep the next horse destined for the same surgery suite. At the
end of the surgery the site is bandaged and the horse is moved to a recovery
stall, where it is hoisted off the bed and onto a recovery mat. Recovery
personnel are called and the tech working on that surgery goes back to the
surgery room to open the room for the next procedure.
One critical point
that keeps this whole process flowing well is communication. Communicating
everything is crucial to being efficient and effective at the job while
maintaining the high standards of the hospital. It’s been a solid two weeks and
I still have a lot to learn about the individual skills and processes that make
this game of ‘surgical Tetris’ (a popular comparison in the clinic) function so
smoothly. That said, I’m making significant progress and I’m looking forward to
the coming weeks and learning so much more.
So, what surgeries have I seen/been in on? A majority of the
surgeries are orthopedic in nature-transphyseal screws, transphyseal bridges,
joint arthroscopies and fracture repairs. I’ve also been in on a postpartum
colic, in which the mare had about 8 feet of dead intestine that required
resection and a jejunocecostomy.



The darker intestine is very likely no longer viable and
requires resection.

Nearing completion, with a successful jejunocecostomy.
Another interesting surgery was a sinus mass removal-the
horse had a bony mass in its sinuses that took up a lot of space!
Warning: sinus surgeries are bloody!

The mass that was removed-hard as bone.
I also had the privilege of being there for a neck plate surgery, where multiple surgeons work together to place a stabilizing plate along the cervical vertebrae of a horse to stabilize vertebral canal and correct some compression of the spinal cord .


Pretty great first couple of weeks!
Subscribe to:
Comments (Atom)