Hello again from beautiful Colorado!
It has been very, very warm this last week in CO. Summer is officially here with temperatures in the 80's and 90's. The other two ICU summer students and I try to get out every weekend and explore a bit of CO. This weekend I think it will involve some sort of swimming to cool off. This last week has been great, lots and lots of colic surgeries, a sinus flap surgery, a few sick foals, and a snake bit case. I haven't learned much about snake bits and how to manage them in vet school, so I am going to share this case and the medical treatments I learned because it was very intriguing to me.
To properly treat snake bites you have to be aware of what venomous snakes are in your local area. Here in CO there are mostly prairie rattlesnakes. At one of our morning meetings I got to speak with a couple of very seasoned field vets who know the CO landscape well. Their insight into where common snake bites are was amazing and really inspired me to get to know the geography and native animals where ever I will be practicing in the future. For example, usually the clinic sees 2-3 snakebites every summer, but some summers they see 10 snakebite cases from just one horse farm. There are quite a few management items that the vets recommend to those farms to help curb the number of bites. The snakes typically like rocky areas, so the vets recommend fencing those type of areas off. One of the older and wise vets even mentioned that pigs are able to eat the venomous snakes because they can survive the bites due to their increased body fat percent. So they have recommended adding a few pigs to the fenced in areas as a short term solution.
Horses are usually bitten on the muzzle, occasionally on the distal limbs, and rarely on their trunk. The muzzle is the most common bite site because they are down grazing and a snake bites them or they see one and go up to investigate it. Sometimes horses step on them and get bite on the distal limbs. One of the vets advised us that if a horse is showing clinical signs of a snake bite, but you can't find the fang marks in the normal locations, it could be because the horse rolled on the snake and was bitten its dorsal spinal area. Usually you will see two bloody fang marks where the snake bite the horse. One of the vets reported seeing a case one time that had bloody fang marks, but the horse didn't have any clinical signs of a snake bite. They contributed this to what is called a "dry bite", where the snake is very young or very sick and doesn't have venom to inject into the horse. The vet recommended still treating the horse with the typical treatment just to be cautious.
The common clinical sign of a snake bite is a massive amounts of swelling in the area that was bitten. Bites to the face are much more severe because they have a greater blood supply to spread the venom. One of the most common issues with a bite to the face is that the swelling mechanically occludes the horses nostrils. A very simple trick to be able to help the horse breath is to insert 1 small section of garden nose into each nostril. This will provide the horse with a patent airway until the swelling can be managed.
The basic treatment for snake bites is to give the horse a steroid, such as dexamethasone, to decrease the swelling and inflammatory reaction. An NSAID, like banamine, can also be helpful to decrease swelling and control pain (NSAID's and steroids should not be given together though, so one or the other). Snake fangs have also been reported to carry bacteria like clostridium, so an effective antibiotic is also a vital part of treatment. Commonly horses that are bitten go into shock, so IV fluids are important to counteract that. If the bite is on a distal limb, a standing wrap and cold hosing can help to decrease swelling. If the bite is on the muzzle, fenestration of the muzzle with a 14 g needle can help to decrease swelling. The area that was bitten should be clipped and cleaned.
The latest development in treating equine snake bites is antivenom. From what the vets explained to us about snake bites, one of the long term side effects can be cardiac damage. This damage can be accessed by measuring troponin, a cardiac muscle enzyme, level right after the bite and a few weeks post treatment. One of the advantages of antivenom is that it might help to decrease the chances of cardiac damage because it neutralizes the toxins. Antivenom is very expensive for equine patients, but if the owner is financially able to afford the treatment, it is recommended. When administering the antivenom, the horse should be carefully monitored for signs of an anaphylatic reaction.
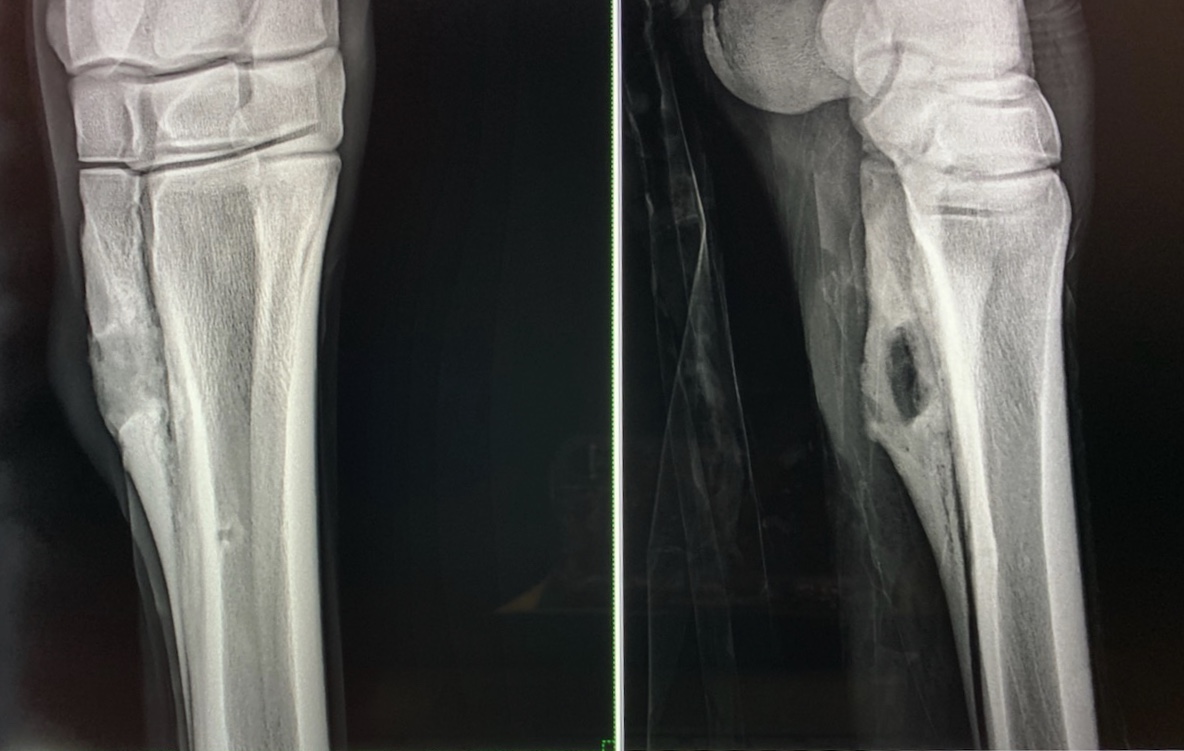
The case I saw managed here was given steroids, IV fluids, broad spectrum antibiotics, and antivenom. Cold hosing and stack wraps were also applied because the bite was on the LF distal limb. The clinicians also emphasized knowing important structures around the bite site because if a joint or tendon sheath is involved that would require more intensive treatment.
The venomous snakes here in CO do not produce a neurotoxin, but snakes in other areas of the country do and that specific envenomation requires a specific treatment.
The biggest lessons I learned about snake bite management in equine patients is that it is a medical emergency that needs to be treated quickly and effectively. Another big take away for me was to know the venomous snakes in your practice area because that will impact your treatment strategy.
Thanks again for reading along and please let me know if you have any questions (denneyk1@msu.edu). I continue to have a great time here in CO and will be back next week with more cool cases.
Best,
Kaity