My first week here at Saginaw Valley Equine Clinic has flown by, but yet it feels like I've been here forever given all that I have learned in the past seven days! Saginaw Valley Equine is a four doctor practice located in Saginaw, MI. Dr. Cumper owns the practice and sees appointments as well as travels to high level horse shows all of the MI and the country. Dr. Jones sees most of the ambulatory cases as well as being responsible for mares and foals. The hospital is equipped with a foal alert system which calls Dr. Jones as well as Diana, one of the techs, and whoever is on call, which this week was me. If a mare is in labor, Dr. Jones arrives in minutes to assist. Dr. Rapson is responsible for most of the reproductive aspect of the clinic. She monitors the reproductive status of the mares at the recip mare farm and times the mares reproductive cycle to be ready for various embryo transfers as well as inseminates and scans (ultrasounds) mares to check for pregnancy. Lastly, Dr. Williams, the Board Certified Veterinary Surgeon performs the surgeries that take place. This varies from colic to arthroscopies and ovariectomies and more. She also sees office visits and is available for farm calls.
My week began when Elaine and I arrived at the clinic for orientation and our first day on Monday. But typical to our profession, we were immediately rescheduled to go out on a farm call to relieve choke in a mammoth donkey. Dr. Jones passed an NG tube and lavaged the esophagus to relieve the choke. It was a messy first call of the day, but the choke was relieved and the donkey should do fine.
After relieving the choke, we also took a look at some smaller donkeys that had just been rescued with extremely overgrown hooves. It will be a long process to recovery, but Dr. Jones recommended some pain prevention and the farrier will soon get to work on relieving the "elf feet."
Since our first time out, Elaine have been on separate shifts. I work 10:30 - 7 and then am on call for the entire week as well as perform treatments during the weekend. Elaine has been working the morning shift. She comes in at 7:00 and works until 3:30, but then is not required to be on call. Next week we will switch.
Throughout the week I have seen a variety of cases. I've seen stallions collected and embryos transferred from a donor mare to a recipient mare. I've assisted with lameness exams including nerve blocks and radiographs. I've helped with pre-purchase exams, which include a standard 20 radiograph study and additional radiographs performed in problem areas.
One case that interested me was a gelding that had chronic nasal discharge and had seen a couple vets before ending up at Saginaw Valley. We performed an endoscopy and Dr. Jones had a lot of trouble entering either guttural pouch, but was getting a lot of mucous on her probe whenever she tried to enter them. This prompted her to take a radiograph of the guttural pouches, where she found a large number of chondroids. Chondroids occur when there is an infection in the guttural pouch and the pus consolidates and can only be removed via surgery. Unfortunately the surgery is not only very costly, but also comes with a high risk of damaging the nerves and arteries that run through the guttural pouch, thus causing nerve damage and possibly even a fatal bleed.

Helping doctors and watch them work through a case is one of the best ways to learn. I've also gained a massive amount of experience giving treatments to various horses. From foal handling to controlling problems animals gaining experience is invaluable. It's also really helpful to actually be the one administering medication and fluids, because understanding why I'm giving a particular medication or treatment helps me to remember it in the future. One case that has caused me to gain a particularly large amount of experience was a dummy foal that came in. The foal had low IgG and elevated Creatinine, indicating failure of passive transfer and possible kidney damage. The foal was not able to get up or down on it's own and it's suckling reflex was inadequate, causing it to be at high risk for aspiration. An NG tube was placed so that the foal could be tube fed until it was able to nurse successfully on it's own. The mare was milked and the foal was fed every two hours throughout the day and night. The foal was also put in fluids to try and flush the kidneys. Maintenance fluid rate for a foal is 100 ml / kg. The foal weighed about 100 lbs (45kg), and was push on a rate of 1 1/2 x maintenance. Accounting for the milk the foal was being given, this meant that the foal was receiving 1 L of fluids every 4 hours for a total of 6 L /day. Additionally, the foal was given Ceftiofur (Naxcel) to fight off any infection. Although all these treatments required TONS of work, the investment is invaluable. The foal is doing much better. Her IgG and Creatinine are back to normal and she is now able to nurse on her own.
The other great thing about spending TONS of time in the clinic is that I was there when a mare began foaling, so I was able to watch the entire process (from a distance)! She had a normal labor with a healthy colt, and seeing the entire process is a wonderful opportunity!

I can't wait to start a new week! Thanks for reading!
-Kaitlin







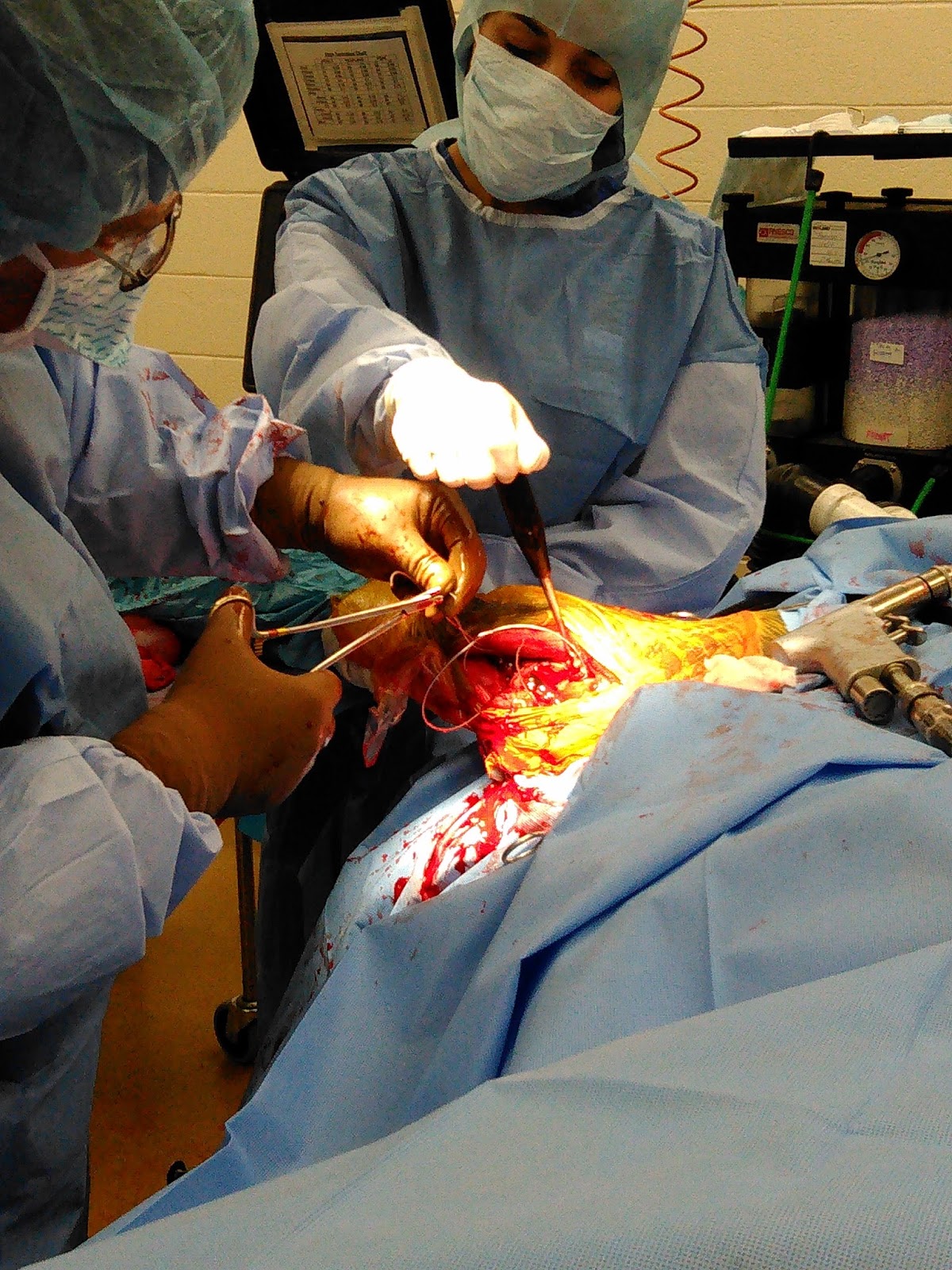












 Incision for c-section!
Incision for c-section! Uterus with cecum on left side of picture!
Uterus with cecum on left side of picture!
































